Introduction
Worldwide, as well as in Australia, many challenges to achieving a sustainable, resilient built environment have been identified, including multidimensional resourcing constraints, rapid urbanisation, failing infrastructure and socio-demographic change.1 Populations are known to be ageing, human diversity is increasingly recognised, and evidence that the built environment affects health and well-being is mounting.2 The ‘neighbourhood’ as a key spatial and social construct, and focus of policy and practice, has received attention across many fields, for example planning, community development, health and sustainability.3 Obviously, the neighbourhood built environment is used by people with disability. Nonetheless, the accessibility performance of the existing built environment, particularly at neighbourhood scale, continues to fail people with disability.4
However, in something of a parallel universe, much built environment assessment research is being undertaken. Many city-enhancement movements, sustainability indicators and built environment performance measures already exist. Improving built environment ‘sustainability’ performance, via measurement, receives much contemporary attention.5 Within the associated bodies of literature, the need to research, critically appraise and measure the existing built environment is well established. Why, then, is built environment accessibility performance at neighbourhood scale for people with disability so rarely considered?
This paper endeavours to respond to this question. First, a brief review of building performance measures, urban realm assessment, and interdisciplinary health-built environment analysis is presented. Second, the lack of engagement with people with disability in relation to accessing neighbourhoods, and the resultant poor built environment accessibility performance, are discussed under the headings ‘design’, ‘planning’ and ‘politics’. Last, the case for assessing neighbourhood accessibility performance, an essential component in the process of built environment accessibility improvement, is put forward.
Built Environment Performance Measures
The performance of residential and commercial buildings and/or their components is already measured in a myriad ways, in Australia and elsewhere. Such tools range from measuring the performance of particular aspects of singular building componentry, including appliances, through to comprehensive investigations of total building systems, albeit from specific perspectives. Furthermore, measurement systems have been in place for decades. In Australia, major household appliances have been star-rated since the mid-1980s.6 More recently, in September 2018, and aimed at global scale, the Net Zero Carbon Buildings Commitment officially launched.7 Backed by the World Green Building Council (WGBC), the project requires signatories to instigate national net zero carbon rating tools and certification schemes by 2030 and commit to all (100 per cent) buildings within their portfolios being net zero carbon by 2050.8
Energy rating systems aimed at improving energy efficiency and/or reducing operating costs within buildings started gaining traction worldwide in the early 1990s. A unifying feature of these systems is benchmarking and rating, permitting succinctly communicated comparison across differing installations and (numerical) ‘incentives’ to do better. Some common examples of such systems are noted in Table 1. Current iterations of such tools are invariably more sophisticated (technical) and/or comprehensive (sustainability-oriented) than when first released.
As alluded to above, the concept of ‘energy efficient buildings’ has morphed through ‘environmentally green building’ and has, more recently, embraced broader readings of ‘sustainability’, including a greater recognition that people inhabit buildings. Developing from a theoretical idea that emerged in the mid-1990s, the Living Building Challenge (LBC, the Challenge) was codified and launched in late 2006.23 The Challenge – with its seven performance areas of Place, Equity, Water, Beauty, Materials, Health + Happiness, and Energy – is considered one of the most onerous, multidimensional building performance tools currently in use.24 Life cycle assessment (LCA) originated out of project-based 1960s and 1970s energy analysis, moved through policy-based applications in the 1990s, and was mainly concerned with environmental impacts in the 2000s.25 LCA is, however, ever-divergent and evolving; a current focus includes life cycle sustainability analysis (LCSA) covering the people (social), planet (environmental) and prosperity (economic) dimensions of sustainability.26 Although early on, in the early 1990s, indoor air quality (IAQ) was predominantly a concern of heating, refrigerating and air-conditioning engineers (HRAEs), the field has subsequently broadened out to consider indoor environment more holistically. Now, using standards and methodologies such as the British Standard BS ISO 17772, Indian Standard ISHRAE Standard 10001: 2016 – Indoor Environmental Quality Standard, and the Building Occupants Survey System Australia (BOSSA), indoor environmental quality (IEQ) is assessed in terms of thermal comfort/temperature, fresh air/indoor air quality, daylight/lighting/lighting comfort, and acoustics/acoustic comfort.27 Further, building occupant well-being is now studied through methodologies such as the WELL Building Standard.28 Grouped under its eleven ‘concepts’ of: Air, Water, Nourishment, Light, Movement, Thermal Comfort, Sound, Materials, Mind, Community and Innovation, the ambit of the WELL Building Standard (v.2 pilot) is wide.29 Most unusually, but very encouragingly, disability is acknowledged, universal design (UD) is referenced, and accessibility requirements are noted.30
Formal assessment via any of the tools mentioned above requires significant financial outlay as assessment is, almost without exception, undertaken by accredited experts using specialised computer software. The shortcomings of ‘one-off’ sustainability assessment tools, and the mismatch between ‘as designed’ ratings and ‘as built’ performance, is coming under increasing scrutiny; ‘set and forget’ is insufficient – evaluation of actual performance, and ongoing monitoring, is required.31 Enriched post-occupancy data collection, more in-depth behavioural studies, and more sophisticated monitoring activities, enhanced by ever-developing computerised analysis systems, are anticipated to improve built environment-human interaction sustainability outcomes.32 Building accessibility, however, is usually ‘compliance’ access-audited against enigmatic legislation, and presented in esoteric spreadsheet format, without any overarching narrative outlining the significance of the individually itemised entries.33 Conventional access auditing, also usually undertaken by accredited experts for a substantial fee, also does not accommodate monitoring, or the collection of post-investigation user satisfaction data, or sophistication of computerised analysis systems, particularly those involving GIS.
Urban realm measurement interests are wide-ranging. Assessing and/or ranking city-scale sustainability, resilience, liveability, smartness and more, is now well-entrenched (see, for example, EIU’s Livable Cities, Mercer’s Quality of Living, AT Kearney’s Global Cities Index, Smart Cities, Resilient Cities, Healthy Cities, and Age-Friendly Cities). Non-standardised evaluation methodologies are, however, cited as a problem.34 Nevertheless, irrespective of specific methodology, the core beliefs of resilient cities evaluation, for example, are: first, that to become more resilient, improvement is needed; second, that existing conditions measurement, via indicators, is an essential precursor to improvement; and third, that cross-sectorial and interdisciplinary collaboration is required.35 Healthy cities evaluation (why, what, for who, by who and how) is also an ongoing thorny issue, but comprehensive problem mapping at the outset leads to enhanced project and participation outcomes.36 Ethical cities measurement processes are still embryonic, but both ‘objective’ quantifiable measures and more qualitative measures involving engagement, judgement and discussion have their valuable places in measurement.37 Therefore, although multiplicity of assessment methodologies is questioned, measurement and collaboration across multiple domains is essential. Disturbingly, however, the need for ‘accessibility in the built environment’ improvement for people with disability is rarely mentioned directly, if at all.
From at least the late 1970s, improving transport infrastructure and public transport has been on the research agenda. Systematically investigating existing physical conditions and policy contexts, development of evaluation methodologies including indices, interdisciplinary collaboration, and stakeholder engagement at local citizen level are all common components of road re/construction, road safety auditing, ‘safe system’ traffic safety, ‘shared space’ design, ‘roads as places’, and mobility.38 In the public transport field, although motivations for desired improvements are manifold, and initiating entities across multiple modes diverse, common tasks include acquiring quantitative data; ascertaining physical, disciplinary and political interconnections; and understanding the existing condition of public transport built assets.39Again, a worryingly common feature of these endeavours is the lack of inclusion of the lived experience of people with disabilities.
Much mapping and modelling, including computer-generated spatial investigations using GIS software, has been undertaken throughout the world.40 Sidewalk details, however, are still commonly missing from GIS datasets.41 Modelling for fire engineering (in dense built-up areas) has been developed.42 Sustainable mobility has been indexed.43 Investigating walkability, measuring urban form complexity, assessing sustainable urban design, and examining crash severity and streetscape design, are common, contemporary, areas of in-depth built environment performance research occurring at neighbourhood scale.44 Improving existing roads, improving road safety, and designing shared pedestrian-vehicle space routinely involves systematically investigating existing physical conditions, evaluating policy frameworks, and community engagement.45 Nevertheless, the urban realm accessibility needs of people with disabilities are rarely considered, and their direct input is rarely sought.
Within the interdisciplinary health-built environment field, scrutinising the built environment at micro-scale (buildings), meso-scale (neighbourhood) and macro-scale (city-wide) is also well established. Often undertaken from multidisciplinary perspectives, there has been much analysis, particularly within the last decade, involving researching, imaging, recording and measuring the interaction between people and their environments, with a view, for example, to increasing physical activity, obtaining insights into older adults’ mobility and well-being, enhancing active travel, reducing negative impacts on health at home, and increasing positive impacts on health at the community level.46 The need to view the ‘problem’ at the scale of the user, and from a user-centred vantage point is acknowledged.47 But, Appleyard, for example, continues the entrenched tradition of highly technical transport-land use evaluation undertaken by experts only; no lived experience and/or community member input is sought, and no concern for the specific travel needs of people with disability is expressed. The key recommendations of health-built environment projects for future research often include focusing on changing existing environments and pursuing interdisciplinary understanding.48 Nevertheless, although terminology such as ‘social inclusion for all’ (or similar) is becoming more common, the need for improving ‘accessibility in the built environment’, for people with disability, is still rarely, if at all, directly mentioned.
Accessing the Neighbourhood?
Design
Existing built environment inaccessibility can be explained, partly, by the central tenets of historical disability models, such as the charity (institutional) and medical models of disability.49 Under these models, the public profile of people with disabilities was rendered virtually non-existent.50 While outwardly signifying care and protection of the vulnerable other, the charity model, and the similar religious and moral disability models, point to the desire to control, via segregation, ‘deviant members’ of society.51 A core response was the construction of institutions. Therefore, in the context of the built environment, the charity model of disability effectively translates to ‘we don’t have to worry about them, they are put away’ in institutions.52 Often large and imposing, with cavernous dormitories and sited within extensive grounds away from town centres, asylums, a common landmark of the late 1800s and early 1900s in Australia, the UK and the USA, are a clear built-form manifestation of the institutional nature of the charity model of disability.53 Imrie observed that ‘western cities are characterized by a design apartheid where building form and design are inscribed with the values of an “able-bodied” society’54 – a consequence of the charity model’s invisible segregation of people with disability.
Central tenets of the medical model of disability are that, first, a person’s ‘impairment’ can be diagnosed, cured, or at least rehabilitated, by modern medicine and/or medical technology, and, second, that such interventions will be provided by all-knowing professionals.55 The medical model, in a health context, is based on classifying levels of deviance or deficiency compared to a supposedly normative state.56 Similar models, such as personal tragedy model, individual model and rehabilitation model, often used interchangeably, point to the individualised emphasis of the medical model. Such ideology tends to lead to the (unacknowledged) belief among built environment practitioners that the built environment accessibility needs of people with disabilities will be resolved by individual provision of personalised medical intervention and/or assistive technology. For built environment practitioners, therefore, the medical model of disability effectively translates to ‘we don’t have to worry about them, they will be fixed’ or, again, institutionalised.57 A crucial consequence of the once pervasive ideology of institutionalisation, which reached its peak under the medical model, is that much existing built environment, particularly within the public realm, is inaccessible for people with disability.58
Engendered by the low public profile of people with disabilities, conformist societal attitudes, design precedents, weak legislation, and poor understanding of the built environment accessibility needs of people with disability, a significant extent of the existing built environment and public transport infrastructure has been designed within a paradigm of a charity/medical model of disability, albeit unconsciously. Another reading of exclusionist design thinking is provided by Finkelstein and Hunt; their social relational theory concludes that social exclusion of people with disability was an outcome ‘of the materialist landscape of the industrial era’ rendering them economically unviable.59 Viewed through such a lens, design of factories and workplaces, schools, public transport systems and infrastructure was heavily influenced by the attitudes of the designers’ clientele. In contrast, well-known contemporary disability models, such as the social and human rights models of disability, offer insight into the imperative of improving the accessibility of the existing built environment.60
The social model of disability was developed in the early 1980s by Mike Oliver, a British academic and disability activist. As explained by the social model, disability arises from barriers within ‘an oppressive and discriminating society’, rather than from impairment per se.61 In a challenge to the medical model, the onus of response is shifted to society to dismantle barriers that construct disability.62 The social model of disability therefore recognises that disability is not a pre-existing, independent, condition – the built environment is a disabling instrument in itself, that is, the nature and experience of disability is directly linked to the built environment.63
New ways of thinking had also extended to built form. Internationally, postmodernist architecture had started to emerge in the 1960s. However, in the 1980s, the Australian, popular version, was rarely manifested in more than facade form and decoration; little attention was paid to postmodernism’s underlying hallmark concerns of diversity and discrimination. Therefore, urban layouts and building design in Australia remained largely untouched by the concerns of either postmodern social theorists or proponents of the social model of disability, thus remaining as inaccessible as ever.
The currently unfolding human rights model of disability did not spontaneously appear, but rather evolved within a continuum of rights-based thinking.64 In response to an emphasis on rights and deinstitutionalisation, disability research and activism work in the USA precipitated the emergence of the independent living movement in Berkeley, California in the early 1970s.65 On the other hand, Schindler (2015) highlights the discriminatory power, through design and planning mechanisms, that the built environment has had, and continues to have, over people’s lives. Central to the human rights model is that all people have rights, including that of built environment access.66 The human rights model, empowered by the United Nations Convention on Rights of Persons with Disabilities (UNCRPD), specifically draws attention to the wide-ranging nature of the built environment, for example, housing, public buildings, transport and social/cultural/recreational locations.67
In discussing the development towards the UNCRPD, Bruce restates the views of prominent disability studies writers (for example, Zola, Oliver and Hahn) in explicitly problematising inaccessible built environments for people with disability.68 Theresia Degener characterises the inaccessibility of the built environment as a human rights problem, suggesting that disability studies has moved beyond the debate of medical versus social models of disability into a new era: a human rights model of disability era as epitomised by the UNCRPD.69 Notions of spatial inclusion at community level are embedded in the UNCRPD and, as evidenced by Preamble and Article content, the way people are supported to interact with their (neighbourhood) environment is considered crucial.70 The UNCRPD/human rights model of disability presages more obviously defined, and compliance-enforceable, built environment accessibility legislation – the prescriptive Americans with Disabilities Act (ADA, USDoJ 2017), for example, rather than the performance-based Australian Disability Discrimination Act.71
From my ‘accessibility in the built environment’ specialist perspective, I believe that understanding the above concepts is invaluable. Improving built environment accessibility is, however, compromised by the lack of understanding of disability issues, including disability models, by built environment practitioners, and the lack of direct engagement with people with disability and the lack of content in curricula.72 Architects, planners, builders and construction engineers, in Melbourne at least, have virtually no exposure to universal design (UD) at trade, undergraduate, postgraduate or continuing professional education levels.73 In 2015, in Australia, across urban design, planning and architecture, no major built environment design programme at undergraduate or postgraduate level contained universal design, designing for disability, inclusive design, people-centred design or the like as a core course.74 In 2016–18, while technical tutor at a leading Melbourne-based university, I found that only 1–3 students in each design studio group of around 16 postgraduates had previous exposure to disability-related teaching content.
Furthermore, built environment design practitioners – architects, for example – are programmed through entrenched educational systems to view the built environment as a ‘problem’ requiring ‘solving’.75 However, conventional training and conventional, isolationist, built environment problem-solving approaches leave built environment design practitioners ill-equipped for an increasingly complex, interdisciplinary, modern world, particularly a world of urbanised, ageing populations and diverse people with disability.76
Planning
Many people with disability across regions as diverse in resources, geography, politics and culture as the UK, New Zealand, Australia, Canada, the USA, continental Europe, Scandinavia, Asia, the Pacific Islands, the African continent and Latin America, find their everyday environments a daily, overwhelming struggle.77 Common themes are very obvious: social inclusion is stymied by the inability to navigate broken travel chains; built environment elements of greatest concern are housing, the public realm pedestrian environment, and public transport; lack of enforcement of existing legislation is a very significant problem; and inconsistent and/or misinterpretation of existing legislation is also problematic.78 Despite all this, accessibility for people with disability in the urban realm, a realm intimately related to ‘planning’, appears to be a built environment performance measure blind spot.
Relationships between physical locations and design quality, individual buildings and the neighbourhood, conventional planning and modern urban form, global and local contexts, and streetscape design and traffic management are complex.79 Nonetheless, sustainability measurement tools at neighbourhood scale, interdisciplinary sustainability assessment at various scales, and weighted indicators for the purpose of ‘sustainability’ evaluation, are now ubiquitous.80 Ewing, Handy, Brownson, Clemente and Winston (2006) argue that, by way of systemised measurement, quantification of qualitative urban design qualities is achievable.81 Sipe, Mayere-Donehue and Dedkorkut (2011) emphasise the educational value, for both professionals and academics, of measuring urban form via international comparative analyses.82 A common thread running through the literature, however, is the need to critically appraise and measure the existing urban environment. Assessment of urban design qualities and landscape character can, with the appropriate checks and balances, be undertaken by laypeople.83 Therefore non-expert local citizens directly assessing existing conditions for the purposes of improving future outcomes is not a weird idea. But embedding people with disability in assessment processes is, disturbingly, still novel.
Improving urban environments via placemaking is now well established in the urban planning lexicon. Placemaking is based on the idea that ‘places’ are more than mere physical spaces, and, as such, can be considered in planning terms as a kind of ‘performance’ enhancement. Professional disciplines such as landscape architecture and urban design are often intimately involved in the process of placemaking through urban realm planning and design. Local government authorities, in Melbourne and elsewhere, often have ‘place managers’ and/or placemaking teams allocated to particular geographical precincts. Early placemaking proponents were somewhat evangelical. The Project for Public Spaces and Metropolitan Planning Council (2008) claimed, for example, that placemaking ‘has the potential to be one of the most transformative ideas of this century’.84 Albeit not necessarily neighbourhood-scale dependent, the intentionally interdisciplinary notion of placemaking is heavily reliant on the concept of ‘the neighbourhood’.85 A currently unfolding iteration of placemaking is ‘placeshaping’.86 Pugalis posits that placeshaping proponents are less enthusiastic about the end-product focus and deterministic nature of placemaking, believing that the process-focused placeshaping approach will yield superior place quality, ‘a constituent factor in the shaping of places that enriches social experiences and economic interactions’.87
Although application may vary, placemaking principles commonly considered essential worldwide include meaningful community stakeholder engagement and existing conditions evaluation (see, for example, Placemaking Chicago: http://www.placemakingchicago.com/). Placeshaping, however, appears to be somewhat in danger of being hijacked by city shaping, (that is, production of iconic infrastructure invariably undertaken by the big end of town), with a resultant lack of attention to grass-roots, social inclusion planning for people with disability. Nonetheless, infrastructure conventionally considered as vehicular transport infrastructure – roads, for example – is under the placemaking evaluation spotlight.88 If roads are to be considered places, then it is certainly timely to gain deeper understanding of people with disabilities’ current lived experience of both the iconically planned and grass-roots unplanned infrastructure environment.
Social inclusion at community level is considered essential for health and well-being.89 But people with disability ‘can’t get there, can’t get in, can’t get it’.90 From a policy perspective, the neighbourhood is of vital importance in influencing children’s physical activity levels and older persons’ physical activity, health and well-being.91 Poor pedestrian infrastructure limits older persons’ physical activity.92 Independent living in ‘ordinary’ community settings is obviously stymied if the neighbourhood pedestrian environment is inaccessible. Disadvantaged communities tend to exhibit poorer outcomes across a range of health and well-being measures, including physical activity and social exclusion.93 However, the relationship between neighbourhood factors and disability is little researched.94
Politics
Regarding the built environment, people with disability continue to experience lack of meaningful involvement in research, participation in decision-making, partnership equality and direct influence over policy.95 In response, people with disability often form their own, grass-roots, specific-interest, ‘self-advocacy’ groups.96 However, such groups tend to have limited impact, as they rarely have sufficient resources to engage in systemic advocacy, an advocacy model considered more effective for policy change.97 On the other hand, well-resourced, ‘healthy environments’ advocacy tends to encompass improving public transport service levels, increasing active transport, making neighbourhoods walkable, communities healthy, ageing actively, and the like, with scant reference to people with disability.98 ‘Human interaction with the built environment’ research continues to exclude people with disability through design limitation and/or intention.99 Across Europe, disabled people’s organisations (DPOs) believe that people with disabilities’ lived experience of transport, housing, ageing, reasonable accommodations (in education and employment), workplace design and vision impairment is little understood and requires multidisciplinary research involving architecture and design.100 The built environment is significantly under-represented within Australia’s disability research base.101
Emerging partnership concepts such as ‘co-production’ and ‘co-design’ are gaining traction in the public service delivery/social policy/disability studies arena.102 Built environment professionals have, by and large, not heard of such things. Built environment researchers and professionals have not paid much attention to people with disability, nor to their physical, sensory, societal or political interactions with the built environment.103 Furthermore, advocacy for built environment accessibility, usually, merely calls for compliance with relevant anti-discrimination and construction legislation, which, invariably, do not mention ‘the neighbourhood’ at all.
People with disabilities’ right to inclusion is, at face value, enshrined in multiple layers of legislation, including the internationally recognised UNCRPD. By, in effect, requiring all of the built environment to be accessible, the UNCRPD is groundbreaking, but there are several layers of procedure between adoption and legislative ‘standing’ within a country. Although Australia has not specifically incorporated the UNCRPD into domestic law, ratification imposes inherent obligations.104 Within Australia, however, most built environment practitioners are not familiar with the UNCRPD and, worldwide, people with disability continue to experience significant difficulty in accessing the built environment, particularly at neighbourhood scale.105
Political direction, societal norms and entrenched ways of working inform governance structures, which are then reflected in regulatory methodologies.106 In Australia, in built environment longevity terms, built environment accessibility legislation is relatively recent. Historically, various state-based building regulations generally contained some provision for ‘disabled access’. However, the DDA was not enacted until 1992, the Building Code of Australia (BCA, (ABCB 2016)) was not fully adopted nationwide until 1998, Braille and tactile signage requirements were not included in the BCA until Amendment 10 in 2002, and the (Australian) Disability (Access to Premises – Buildings) Standards 2010 (Premises Standards, (Australian Government 2010)) was not in force until 2011!
Furthermore, built environment legislation is opaque.107 As I108 have discussed previously, Australia’s complaints-based DDA provides a broad-brush overarching framework, but makes scant direct reference to the built environment. The (Australian) Disability Standards for Education 2005 (Education Standards) are generally ignored by built environment practitioners and the Disability Standards for Accessible Public Transport 2002 (Transport Standards) and Disability (Access to Premises – Buildings) Standards 2010 (Premises Standards, Australian Government 2010) are incomprehensible to those without sufficient background technical knowledge and access to all referenced documents, the latter not being freely available. Deemed-to-satisfy provisions, in both the Premises Standards and the Building Code of Australia (BCA), are not prescriptive; satisfying the Performance Requirements is the legislative requirement. Significant portions of buildings, for example, fit-out, fixtures and fittings, are not directly covered in deemed-to-satisfy provisions, which mainly focus on wheelchair-accessible paths of travel and toilets. BCA Parts concerning ‘accessibility’ do not reference either the DDA, or Disability Standards. The BCA and the Premises Standards do not cover the public realm pedestrian environment nor most private dwellings, categories of built form spatially comprising most of the built environment and two of the three most common areas of built environment accessibility distress for people with disability.109 As a result, within Australia, built environment practitioners’ understanding of accessibility is limited, tending to devolve into a checklist response to BCA Part D3 clauses.
As noted in this paper and elsewhere, ‘disability’ and ‘built environment’ tend not to mix.110 Built environment accessibility policy is undeveloped, and built environment accessibility legislation is object-centred, implementation-focused, and taken as fact.111 In contrast, as indicated by my current PhD studies, disability legislation and policy tends to be person-centred, policy reasoning explained, and, essentially, a public sector activity. Creating and delivering built environment form is, conversely, increasingly a private-sector activity.112 The actors involved, however, have little understanding of either the accessibility needs of people with disability, or the inaccessibility, particularly at neighbourhood scale, of the existing built environment.
Assessing Neighbourhood Accessibility Performance: Measure
Empirical measurement of the existing built environment, particularly at neighbourhood scale, is lacking.113 As I114 have previously discussed, ongoing development of publicly available access auditing tools is occurring in the USA. Assessment using such tools is, however, invariably compliance-based, in checklist format, and not an easily communicable measure of built environment performance. Compliance-achieving rectification recommendations are the main output, along with cost estimates. Legislation interrogation and user preferences are not contemplated, reducing the process to a financial transaction, rather than an upholding of rights. Data obtained are not applicable at neighbourhood scale, and there is no expectation that findings will be used for any wider, community-oriented, benefit. Contemporary investigations into neighbourhood accessibility appear to have mostly emerged from non-built environment disciplinary perspectives and do not purport to be replicable assessment instruments. While the somewhat illogical nuances of built environment production are difficult to comprehend from a non-built environment perspective, clearly the built environment knowledge domain does not, generally, understand disability.115
Requiring collaboration between the built environment and disability knowledge domains and questioning of existing expert-driven assessment methods, a new tool, the Universal Mobility Index (UMI), has emerged.116 The UMI, as tool, is methodologically intended to function as a rights-based indicator of built environment accessibility for people with disability at neighbourhood scale. The existing built environment, at neighbourhood scale, encompasses a diversity of constructed forms that can be broadly categorised as: infrastructure, public buildings, commercial buildings and private dwellings.117 Drawing on the work of significant urban theorists, including Jane Jacobs and Leon Krier, Saeidi and Oktay state that ‘an ideal neighbourhood that meets all users’ requirements is more likely to be in a format that is widely diverse in terms of form [both built and natural], use and user’.118 Therefore, individually and collectively, countless combinations and permutations of (diverse) people-(diverse) environment interactions transpire in day-to-day travel chains, with resultant impacts on the accessibility rights of people with disabilities.
The UMI is projected by its developers119 to be a powerful advocacy tool for people with disability and their representative organisations, succinctly summarising (by way of a number) the (in)accessibility of the existing built environment at neighbourhood scale and illuminating the policy environment contributing to same. An initial pilot study, testing the UMI and examining its strengths and weaknesses, was conducted in Kensington, Melbourne, Australia in 2011.120 It was broadly established that the tool can generate results and be undertaken in the field, albeit with some challenges.121 Consequently, it was intended that the tool, after immediate further development, be rolled out for use by, primarily, local government and DPOs. However, Green’s terminal illness status precluded further development at that time.
The Universal Mobility Index Tool
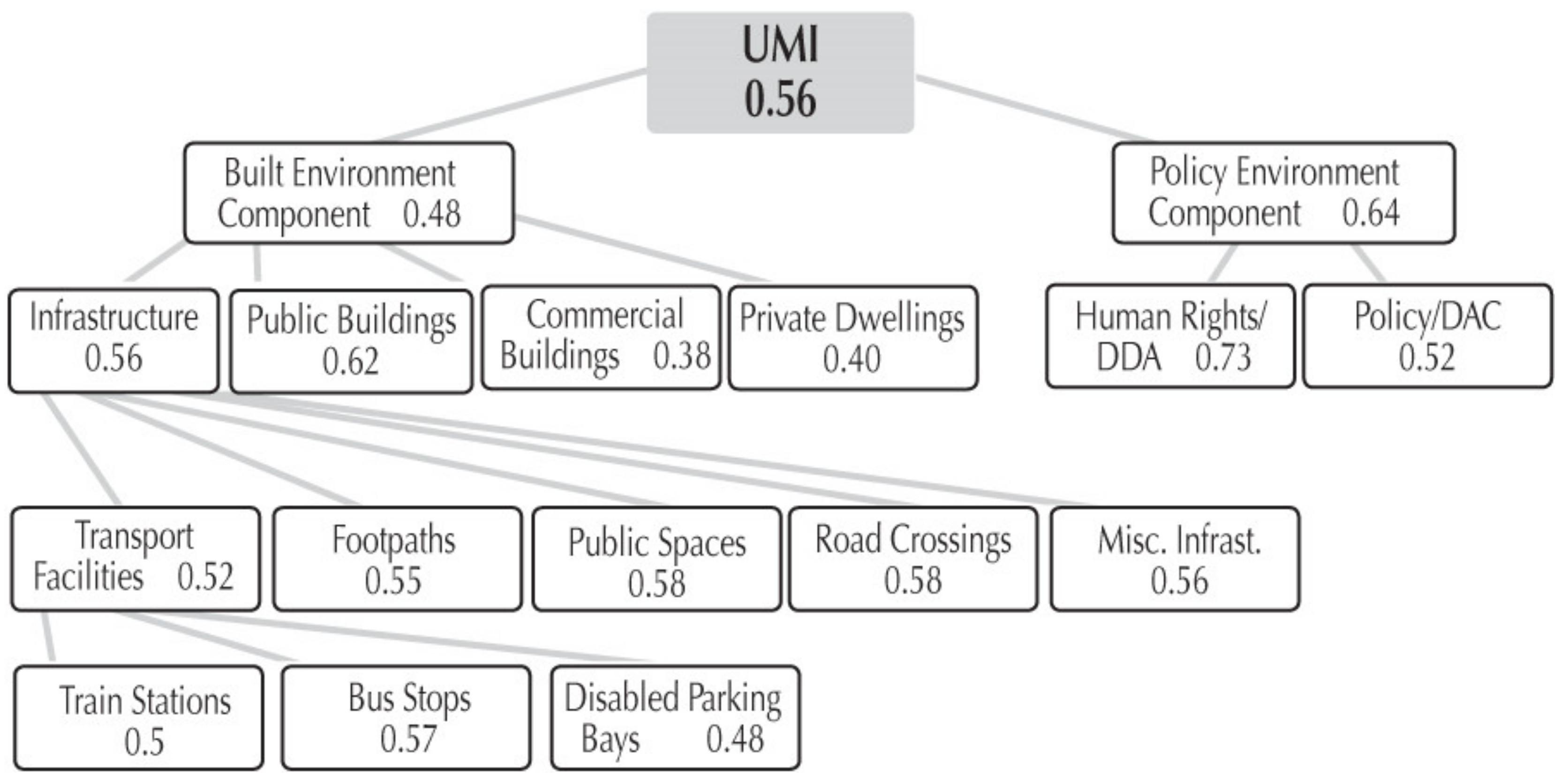
Although ‘human rights model of disability’ was not a common term at either UMI origin or Kensington pilot, the view that people with disability have a human right to fully use the neighbourhood built environment is central. An essential, and defining, feature of the UMI is the dual componentry of built environment and policy environment. These two components are scored, in line with standard indicator-to-index protocols, with resultant values being between 0.00 (very bad, fully inaccessible) and 1.00 (very good, fully accessible). The two component values are then averaged to obtain the (final) UMI score.
The built environment component captures a snapshot of people with disabilities’ lived experience of existing neighbourhood built environment accessibility. Built environment subcomponents are: infrastructure, public buildings, commercial buildings and private dwellings. Infrastructure is further segmented, as are various other subcomponents. Built environment accessibility assessment is undertaken by people with disability themselves, working in teams – another essential, and defining, characteristic of the UMI tool. The policy environment component captures a snapshot of human rights, disability discrimination legislation, and people with disabilities’ effective voice in policymaking in the pilot locality/country. Policy environment subcomponents deal with human rights and legislation, and policy and representation. In contrast to conventional access auditing, policy environment evaluation is essential to UMI application.
Essential stages involved in operationalising the UMI tool are summarised in Table 2.
The Kensington pilot was conducted in accordance with the above format. Built environment elements (n = 2101) within approximately 400–600 m in all directions from Kensington Station were classified and uniquely identified. Random sampling was applied at 90 per cent confidence interval and ±10 error (p < 0.1), and the locations of the sample elements were mapped. The pilot area was divided into segments corresponding to manageable assessment sessions of around 90 minutes. Site assessors, volunteers with a range of differing impairments affecting their mobility, worked in teams and used their own lived experience to come to a consensus on the accessibility of each element inspected. The resultant five-point ‘very bad’ to ‘very good’ Likert-scale data were converted, in line with standard indicator-index protocols, to values between 0.00 (very bad, fully inaccessible) and 1.00 (very good, fully accessible). The built environment component value in Kensington was 0.48. A policy environment questionnaire was distributed to a wide range of local government and NGO/NfP stakeholders; answers were a choice of: ‘yes’, ‘partially’ or ‘no’. This was then converted to an index value between 0.00 (would require all ‘no’ responses) and 1.00 (all ‘yes’ responses). The policy environment component value in Kensington was 0.64. The final UMI score, the average of the built environment and policy environment scores, was 0.56. Weightings were not applied to any score calculations.
Built environment classifications and disaggregations, and index values for both built environment and policy environment and their respective subcomponents, are shown in Figure 1.
Following calculation of all subcomponent scores and final score, participant input was sought regarding prioritisation of advocacy effort; infrastructure was unanimously considered to be the most important.
Concluding Remarks
Built environment performance assessment, in many guises, is already flourishing; it is not a weird idea. Increasingly, assessment is becoming interdisciplinary and multi-domained. The built environment at both the building scale and the urban realm is being investigated, mapped and modelled. Systematically investigating existing physical conditions, evaluating policy frameworks, and engaging the community are all well-established elements of measures aimed at improving built environment performance outcomes. But still, input from people with disability is rarely sought. Without neighbourhood-scale accessibility performance measurement tools aimed at evaluating lived experience, it is difficult to see how a well thought-out, rather than reactionary, programme of neighbourhood accessibility improvement can be determined. Informed by an understanding of the potency of disability models, the Universal Mobility Index offers a potential way forward to measure built environment accessibility performance at neighbourhood scale for people with disability. The validity of this proposition will be tested in further piloting to be undertaken as part of my current PhD studies.