
Introduction
Quality assurance (QA) in radiography is a critical means of ensuring and maintaining high image quality as optimized image quality allows for more accurate diagnosis.(1–3) Radiation protection is important in children who have more radiosensitive organs and have increased risk for radiation induced cancer compared to adults.(1,2,4) To achieve this, paediatric radiology emphasizes ‘diagnostic quality’ over ‘best quality’ (2) with particular emphasis on the dose to be As Low As Reasonably Achievable (ALARA) (5,6) as emphasized in the Image Gently guidelines and campaigns.(6,7)
Quality assurance of paediatric chest X-rays may be compromised in unsupervised radiology units without paediatric trained radiographers or paediatric radiologists.(1–3) Cook et al. recommend that in the ideal setting QA in radiography should be performed on a daily and continuous basis, however, this is not always possible in resource limited environments.(2,3) Following the guidelines outlined in the ALARA principles, good collimation that only includes the field of interest and the use of protective shielding are essential for dose reduction, although these may result in chest X-ray cut-off or obscuring of important structures by the shield in a very mobile child. To address the issue of mobility of children, radiographers sometimes do the opposite and use wide collimation when children are moving and uncooperative.(1) Patient immobilization devices may improve the quality of paediatric chest X-rays in terms of rotation, lordosis and scoliosis but does not have an impact in improving collimation, cut-off and inspiration.(8)
Children are smaller in size and often less compliant than adults which affects the way plain radiographs are performed and the methods employed to optimize dose. With utilization of digital or computerized radiography there is risk of increased radiation exposure as the technique has a wide dynamic range of exposure and thus difficult to maintain ALARA principals.(7) Efforts to reduce dose should not compromise on image quality (7) as paediatric radiographs have relatively low contrast.(5) A constant challenge in paediatric radiography is achieving the balance between acceptable image quality and low radiation dosage. Paediatric patients vary widely in size and weight. This necessitates imaging techniques with a range of different parameter settings for the same anatomical regions, to gain optimal results.(5) Experienced and dedicated staff are the key to quality imaging in children as staff with greater experience are more capable of selecting imaging parameters that will optimize the quality and limit the radiation dose to the paediatric patient.(2,5)
There is a paucity of published literature on paediatric chest X-ray quality and the impact of QA practices in developing countries without paediatric trained radiographers or paediatric radiologists. Comprehensive, standardized multicentre paediatric pneumonia aetiology studies can serve as useful platforms from which image quality trends can be interrogated. To assess quality of chest X-rays we prospectively evaluated chest X-rays from the Pneumonia Etiology Research for Child Health (PERCH) study in 7 developing countries to determine chest X-ray quality over a 14 months period.(9)
Methods
The PERCH study was a prospective multi-centre, international case-control study designed to establish which pathogens are causative of World Health Organization (WHO) defined severe and very severe pneumonia in hospitalized children between 28 days and 59 months of age in middle and low income countries.(9) The PERCH study was conducted in 9 sites (10 hospitals) in 7 countries, namely Bamako (Mali), Basse (The Gambia), Dhaka (Bangladesh), Johannesburg (South Africa), Kilifi (Kenya), Lusaka (Zambia), Matlab (Bangladesh), Nakhon Phanom (Thailand) and Sa Kaeo (Thailand).
Description of the Radiology Department in each of the 7 country, 9 site PERCH Study is detailed in Supplementary Table 1.
Description of the Radiology Department in each of the 7 country, 9 site PERCH Study
| Site (Country) | Hospital Type | Paed Beds | X-ray Unit | Paediatric Trained Radiographers | Children X-rayed with adults | Average no of Pediatric X-rays done per day | X-Rays Reported by radiologist | No of RadiologistsOn Site |
|---|---|---|---|---|---|---|---|---|
| Bamako (Mali) Hospital Gabriel Toure | Pediatric | 143 | Digital | No | No | 15 | Yes | 3 |
| Basse (The Gambia) Basse Health Centre | Adult and Pediatric | 25 | Digital | No | Yes | 12 | No | 0 |
| Dhaka (Bangladesh) Hospital ICDDR, B | Adult and Pediatric | 350 | Digital | No | Yes | 30 | No | 1 |
| Dhaka (Bangladesh) Monowara Hospital | Adult and Pediatric | 32 | Digital | No | Yes | 15 | Yes | 1 |
| Johannesburg (South Africa) Chris Hani Baragwanath Academic Hospital | Adult and Pediatric | 450 | Digital | No | No | 58 | No | 1 (10)* 10 in total |
| Kilifi (Kenya) KEMRI-Welcome Trust Research Centre | Adult and Pediatric | 54 | Digital | No | Yes | 10 | No | 0 |
| Lusaka (Zambia) University Teaching Hospital | Adult and Pediatric | 346 | Analogue | No | No | 40 | No | 3 |
| Matlab (Bangladesh) Hospital ICDDR, B | Adult and Pediatric | 85 | Analogue | No | Yes | 5 | No | 0 |
| Nakhon Phanom (Thailand) Nakhonphanom hospital | Adult and Pediatric | 74 | 6 months Analogue, 8 months Digital | No | Yes | 15 | No | 2 |
| Sa Kaeo (Thailand) Crown Prince General Hospital | Adult and Pediatric | 69 | Digital | No | Yes | 20 | No | 1 |
Each site enrolled cases prospectively for 24 months; South Africa 920 cases, Mali 674 cases, The Gambia 638 cases, Kenya 634 cases, Zambia 617 cases, Bangladesh 525 cases and Thailand 224 cases.
Chest X-ray QA assessment for this study was performed prospectively for all sites over a 14 month period from October 2012 to November 2013. Depending on the study site either digital chest X-rays or analogue chest X-rays that were scanned to a digital format (Supplementary Table 1) were uploaded from each of the 9 sites into an online database (EMMES Corporation, Rockville, Maryland, USA) on a monthly basis during the full course of the study. Only the chest X-ray uploaded during the 14 month chest X-Ray QA period will be described in this study. For the purposes of this study chest X-ray quality was assessed per each site and the city example Johannesburg in South Africa will be referred to.
In 8 out of the 9 sites only frontal chest X-rays were routinely performed in children investigated for pneumonia hence quality assessment was performed on frontal chest X-rays only. In Johannesburg (South Africa) both frontal and lateral chest X-rays was performed in children investigated for pneumonia from this site, hence quality assessment was done on both frontal and lateral chest X-rays. South Africa has a high burden of childhood pulmonary TB (10,11) and superimposed pulmonary tuberculosis (TB) is common in children hospitalized with bacterial or viral pneumonia.(12,13) Routine lateral chest X-rays are performed in children investigated for pneumonia in South Africa as they may improve the detection of lymphadenopathy in children investigated for pulmonary tuberculosis.(14)
From the monthly uploads to the EMMES Corporation STATA software (StataCorp, College Station, Texas, USA), 10 chest X-rays were randomly selected from each of the 9 study sites every month during the study period, for quality evaluation for this study.
Over the 14 month study period an external paediatric radiologist (VM), assessed chest X-ray quality with a customized forced choice tick sheet using 6 parameters developed from the European guidelines on quality criteria for diagnostic radiographic images (15) and the modified parameters developed by Cook et al.(2) The 5 parameters assessed included positioning, collimation, exposure, inspiration and processing and are described in Table 1. For processing we included problems with scanning analogue chest X-rays to a digital format. For the 6th parameter, presence or absence of motion ‘yes’ or ‘no’ was assigned. The external reviewer was blinded to all the clinical information, except the month of chest X-ray examination and the study site.
Customized Chest X-ray Quality Assurance Assessment
| Parameter | Good | Fair | Bad |
|---|---|---|---|
| Positioning | Perfectly straight | Mild rotation but diagnostic | Marked rotation and non-diagnostic |
| Collimation | Optimum Collimation | Wide collimation but not including other body parts | Wide collimation including other body parts/organs or over collimation with normal chest anatomy cropped |
| Exposure | Optimum with visualization of trachea, main bronchi and vascular pattern in two-thirds of lungs | Suboptimal only major anatomy visible but diagnostic | Either overexposed or underexposed and non-diagnostic |
| Inspiration | Well inspired > 6 anterior ribs | Under inspired < 6 anterior ribs but diagnostic | Under inspired < 6 anterior ribs and non-diagnostic |
| Processing | Optimum | Suboptimal (eg: roller marks from processor) but diagnostic | Non diagnostic |
The external radiologist chest X-ray quality assessment reports were sent back to each site on a monthly basis. This individual site feedback was designed so that each site/radiology department could identify problematic parameters in maintaining chest X-ray quality and identify areas for improvement by providing feedback to radiographers and radiologists in their respective departments. The individual sites were also asked to provide feedback to the monthly chest X-ray quality assessment reports. Challenges and limitations in obtaining good chest X-ray quality were thus identified in each site.
For the purposes of the current report, specific QA interventions and responses for each PERCH study site were evaluated through communication with the radiologist/clinician responsible for chest X-ray data collection and quality control at each PERCH site by the principle investigator of this study (NM). The site specific interventions were verified by the external radiologist (VM). These included training of radiographers, chest X-ray quality checks performed weekly by radiologist, monthly feedback on PERCH QA reports given to radiographers and PERCH quality feedback recommendations applied across the board and are summarized in Supplementary Table 2 at the various sites.
Chest X-ray Quality Assurance Activities at Each of the 9 Sites
| Site (Country) | Chest X-ray Quality Assurance Activities at Each of the 9 Sites |
|---|---|
| Bamako (Mali) | Training of radiographers on CXR QA at start of study and at 6 monthly intervals. Chest X-ray quality checks performed weekly by radiologist. PERCH CXR QA report feedback given to radiographers as a group on a monthly basis. Six months into the study all CXRs were assessed for diagnostic and quality assessment. |
| Basse (The Gambia) | Existing QA program for all radiographs performed in department. Training and supervision of radiographers performed by senior radiographer from MRC including quality control of a random selection of radiographs every 3 months. Reading of all CXRs for diagnostic and quality assessment done by study clinicians, feedback in real time to radiographers on quality. Feedback to radiographers on PERCH reports monthly. |
| Dhaka ICDDR, B (Bangladesh) | Monthly discussions of the PERCH CXR QA reports with the radiographers and radiologist in the radiology department, with group and individual feedback. PERCH CXRs read by PERCH study clinicians using a customized report, with feedback to radiographers. |
| Dhaka Monowara (Bangladesh) | Routine reporting of all plain radiographs by radiologist. PERCH CXR QA monthly feedback given to radiologists and radiographers at this site. |
| Johannesburg (South Africa) | Dedicated radiographers allocated to paediatric radiology department during office hours. Discussion of the monthly PERCH QA reports with the radiographers in the paediatrics radiology department. Approximately 10% of PERCH CXRs read by radiologist using a customized report and feedback on CXR quality given to radiographers at informal meetings during study. |
| Kilifi (Kenya) | Monthly CXR QA meetings, regarding PERCH feedback. Individual feedback as radiographers had to sign against all plain radiographs they performed. PERCH quality feedback recommendations applied across the board, since they were generalizable to all radiographs. |
| Lusaka (Zambia) | Each month the PERCH QA reports were discussed with the chief radiographer and radiographers in the department. Feedback on CXR quality was both done individually and as a group and focussed on characteristics of ‘good’ quality images, and the mistakes that led to the ‘poor’ quality images. Radiographers with more experience in paediatric imaging trained junior radiographers in portable analogue X-ray unit usage in children. Damaged and dirty screens were cleaned or replaced during the course of the study. |
| Matlab (Bangladesh) | Discussion of the PERCH QA reports with the one radiographer on site every month. PERCH CXRs read by PERCH study clinicians using a customized report and feedback on quality of CXRs given to radiographer. |
| Nakhon Phanom (Thailand) | Monthly feedback on PERCH QA reports given to radiographers. Overexposure to abdomen and pelvis was one of the site's concerns: study procedures were communicated with paediatricians, radiologist and radiographers. PERCH study clinician assessed PERCH CXR quality and provided routine feedback to radiology department. |
| Sa Kaeo (Thailand) | Plain radiographs not routinely read by radiologist. But all PERCH CXRs were routinely reported by on site radiologist and feedback was given in real time to radiographers on CXR quality. Monthly feedback on PERCH quality reports that where sub-optimal given to radiographers and these CXRs quality errors were discussed. |
For each of the 5 parameters of positioning, collimation, exposure, inspiration and processing an arbitrary score of 2 = good, 1 = fair and 0 = bad was assigned. For the 6th parameter motion an arbitrary score of 1 = no motion and 0 = motion was assigned. The maximum score that chest X-rays were assessed was out of 11. To evaluate the effect of QA activities in each of the 9 sites over the 14 month period, a test for trend analysis was performed using the combined arbitrary scoring system on a month to month basis. The number and percentage of good, fair and poor chest X-rays for each of the 6 parameters as delineated in Table 2 was determined for each site. The impact of the PERCH chest X-ray QA activities was inferred by conducting a test-for-trend analysis for the combination of all 6 parameters during each month of the study. This was done on a site-by-site basis.
Combined 9 Sites Results for each Parameter
| Parameter | Good N (%N) | Fair N (%N) | Bad N (%N) |
|---|---|---|---|
| Positioning | 691 (92.50) | 54 (7.23) | 2 (0.27) |
| Collimation | 560 (74.97) | 154 (20.62) | 33 (4.42) |
| Exposure | 578 (77.38) | 145 (19.41) | 24 (3.21) |
| Inspiration | 684 (91.57) | 54 (7.23) | 9 (1.20) |
| Processing | 623 (83.40) | 105 (14.06) | 19 (2.54) |
| Parameter | No N (%N) | Yes N (%N) | |
| Motion | 658 (88.09) | 89 (11.91) |
Ethics approval for use of the chest X-ray QA data from all 9 PERCH sites, 7 countries’ was obtained from the Johns Hopkins School of Public Health IRB approval No: 0000307 and the PERCH Executive Committee.
Results
A total of 747 chest X-rays in 9 sites (range of 44-119 per site) had quality assessment using the customized force choice reporting system; Supplementary Table 3. In 8 out of the 9 sites quality assessment was performed on frontal chest X-rays only, and in Johannesburg (South Africa) quality assessment was performed in 81 (68%) frontal and 38 (32%) lateral chest X-rays. There was no statistically significant difference between the quality of frontal compared to lateral chest X-rays (p = 0.274) in Johannesburg (South Africa) using the customized quality assessment.
Number of Chest X-rays with Quality Assurance Assessment in each site
| Site (Country) | Total Number of CXRs that had quality assessment over 14 month period | Total number of CXRs loaded on EMMES Corporation, over 14 month study period | Percentage of CXRs that had quality assessment over 14 month study period |
|---|---|---|---|
| Bamako (Mali) | 64 | 295 | 22% |
| Basse (The Gambia) | 90 | 455 | 20% |
| Dhaka (Bangladesh) | 85 | 151 | 56% |
| Johannesburg (South Africa) | 119 | 811 | 15% |
| Kilifi (Kenya) | 70 | 297 | 24% |
| Lusaka (Zambia) | 117 | 253 | 46% |
| Matlab (Bangladesh) | 79 | 250 | 32% |
| Nakhon Phanom (Thailand) | 79 | 110 | 72% |
| Sa Kaeo (Thailand) | 44 | 56 | 79% |
In Johannesburg (South Africa) a large total number of chest X-rays (n = 811) were performed and uploaded over the 14 month study period, hence 15% (119/811) of chest X-rays had quality assessment. This percentage is considerably lower than the Nakhon (Thailand) and Sa Keo (Thailand) sites where 72% (79/110) and 79% (44/56) of radiographs performed respectively, had quality assessment due to the lower total number of chest X-rays that were performed and uploaded over the 14 month study period.
In all 9 sites a low percentage (0%–11%) of chest X-rays were reported as bad in the 5 parameters: positioning, collimation, exposure, inspiration and processing using the customized chest X-ray reporting system. Motion was present in 0-23% of chest X-rays.
Two out of the 9 sites i.e.: Dhaka (Bangladesh) and Kilifi (Kenya) scored above 80% for each of the 6 parameters assessed in the customized chest X-ray quality assessment. These 2 sites had the best chest X-rays quality assessment results. Figures 1a-1f.
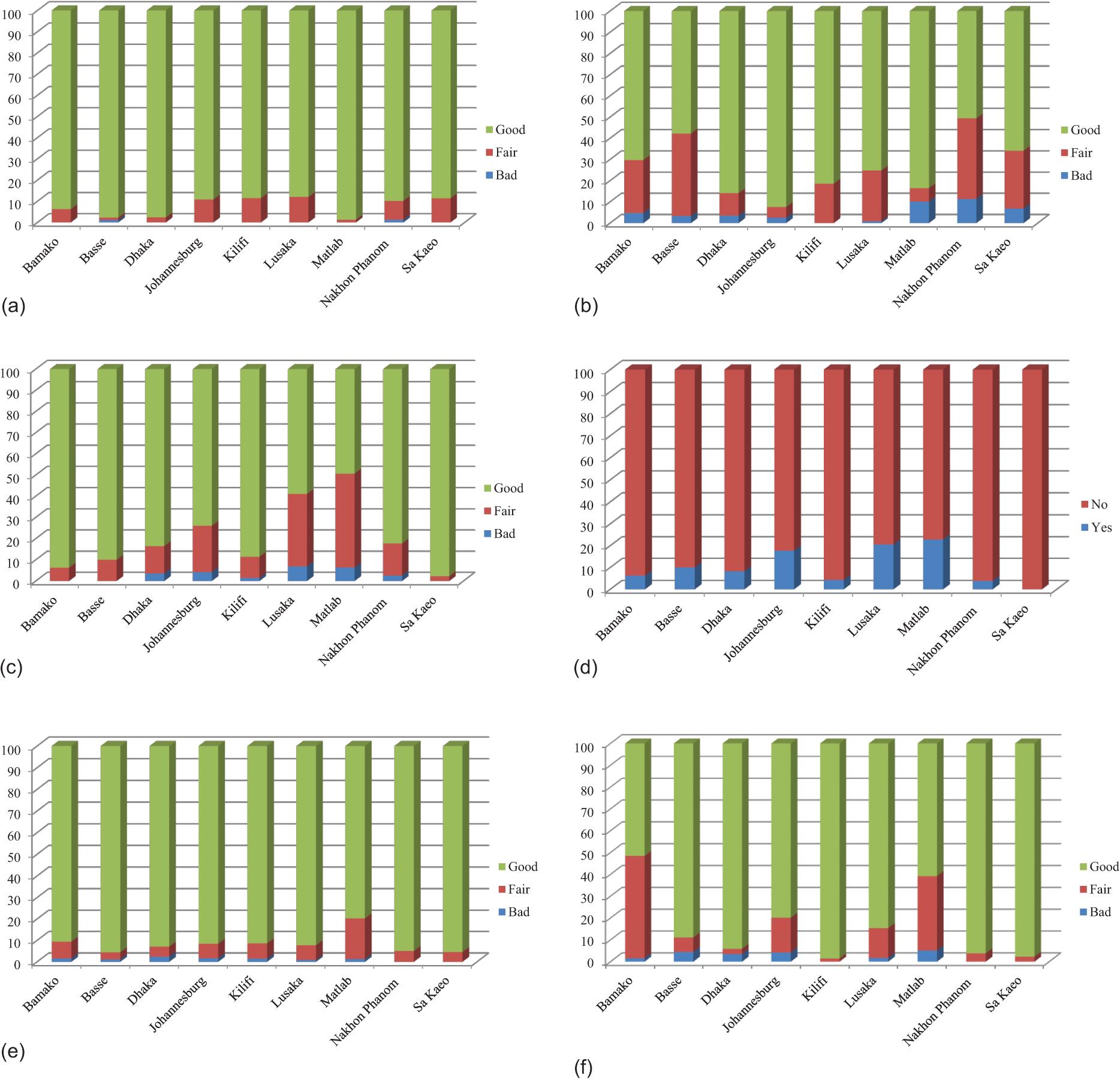
(a)Positioning; (b) Collimation; (c) Exposure; (d) Motion; (e) Inspiration and (f) Processing
Three out of the 9 sites, Basse (The Gambia), Nakhon (Thailand) and Sakeo (Thailand) scored above 80% for all parameters except collimation. In Basse (Gambia) 58% scored good, 39% scored fair and 3% scored bad for collimation. In Nakhon (Thailand) 51% scored good, 38% scored fair and 11% scored bad for collimation, while in Sa Kaeo (Thailand) 66% scored good, 27% scored fair and 7% scored bad for collimation using the customized chest X-ray quality assessment. Figures 1a-1f.
One out of the 9 sites, Johannesburg (South Africa) scored 80% and above for all parameters assessed in the customized chest X-ray quality assessment except exposure. In Johannesburg (South Africa) 74% scored good, 22% scored fair and 4% scored bad for exposure.
Bamako (Mali) scored 90% and above for 4 parameters: positioning, exposure, motion and inspiration. Bamako (Mali) scored 70% good, 25% fair and 5% bad for collimation and 51% good, 47% fair and 2% bad for processing using the customized chest X-ray quality assessment. Figures 1a-1f.
Lusaka (Zambia) scored 80% above for 4 parameters positioning, motion, inspiration and processing. Lusaka (Zambia) scored 75% good, 24% fair and 1% bad for collimation and 59% good, 34% fair and 7% bad for exposure.
Matlab (Bangladesh) scored 80% and above for 3 parameters: positioning, collimation and inspiration. Matlab (Bangladesh) scored 50% good, 44% fair and 6% poor for exposure, 61% good, 34% fair and 5% bad for processing and 77% no motion and 23% motion. Figures 1a-1f.
Combining the results of all 9 sites, collimation performed the worse with 20% assessed as fair and 4 % bad. Positioning and inspiration were the parameters that the sites performed the best with 93% and 91% assessed as good respectively. Results are summarized in Table 2. A low percentage 0%-4% was assessed as bad, making the chest X-ray uninterpretable. Overall, 12% of films had motion artifact.
The test for trend analysis for the median quality assessment score was performed for each of the 9 sites. (Supplementary Table 4) Chest X-ray QA activities made a significant impact in improving chest X-ray quality in 3 of the 9 sites over the 14 month period with a statistically significant improvement of chest X-ray quality for Matlab (Bangladesh) p < 0.001, Johannesburg (South Africa) p < 0.035 and Nakhon (Thailand) p < 0.001 None of the 9 sites showed a statically significant worsening of chest X-ray quality over the14 month period as determined by the test for trend analysis. The graphic representation of the combined 9 site chest X-Ray quality score over the 14 month study period using test for trend analysis is demonstrated in Figure 2.
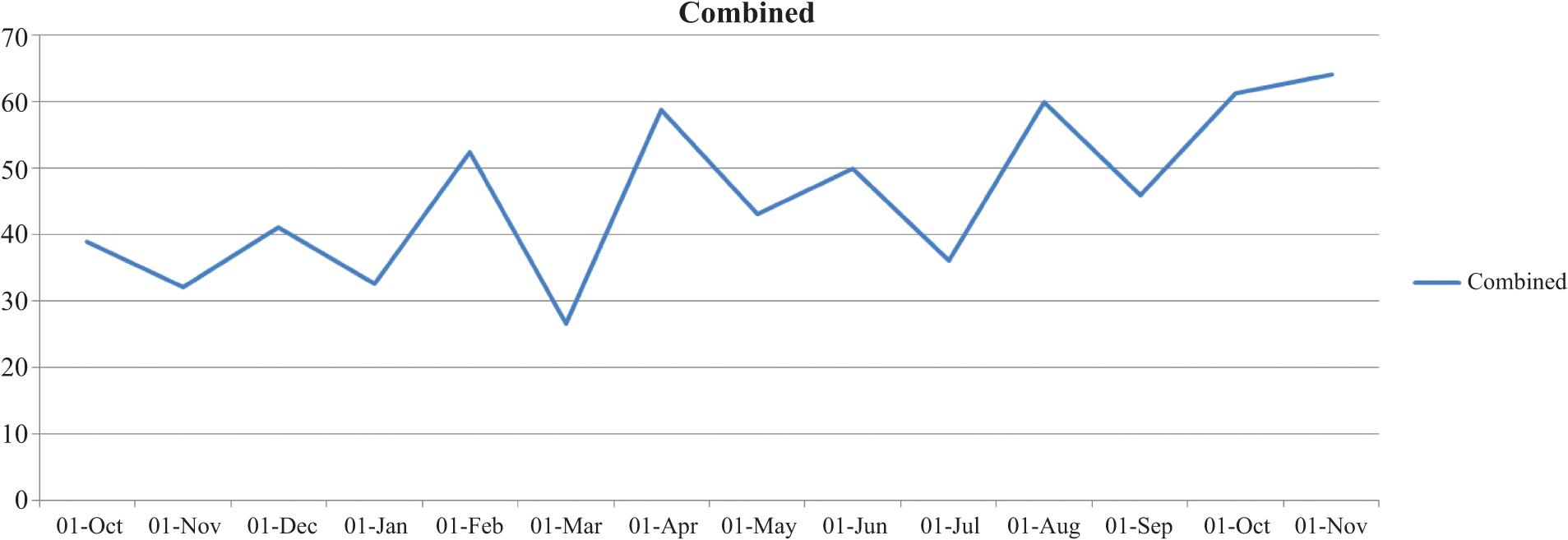
Graphic representation of combined 9 site Chest X-Ray Quality score over 14 month study period
Chest X-ray Quality Time Series Analysis over 14 month period for each of the 9 sites using Test for Trend
| Site (Country) | Median QA Score out of a total of 11 per Month | P value | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | ||
| Bamako (Mali) | 10.5 | 11 | 9.5 | 9 | 10 | 10.5 | 10 | 0.426 | |||||||
| Basse (The Gambia) | 10 | 10 | 11 | 10 | 11 | 9 | 11 | 10 | 11 | 0.089 | |||||
| Dhaka (Bangladesh) | 11 | 11 | 10 | 10.5 | 11 | 10 | 11 | 11 | 11 | 9.5 | 10.5 | 11 | 11 | 0.659 | |
| Johannesburg (South Africa) | 9.5 | 10.5 | 9 | 10 | 10 | 10 | 10 | 11 | 10.5 | 11 | 11 | 10 | 0.035 | ||
| Kilifi (Kenya) | 10.5 | 10 | 11 | 11 | 11 | 11 | 11 | 0.831 | |||||||
| Lusaka (Zambia) | 10 | 10 | 10 | 10.5 | 11 | 9 | 10 | 9 | 10 | 9 | 11 | 10 | 0.890 | ||
| Matlab (Bangladesh) | 9.5 | 6.5 | 8.5 | 9 | 9 | 8.5 | 9 | 10 | 10 | 11 | 11 | <0.001 | |||
| Nakhon Phanom (Thailand) | 10 | 9.5 | 9 | 9.5 | 10 | 9 | 11 | 10.5 | 10 | 11 | 11 | 11 | 11 | 11 | <0.001 |
| Sa Kaeo (Thailand) | 10.5 | 11 | 11 | 10 | 10.5 | 11 | 11 | 11 | 11 | 11 | 10 | 10 | 10.5 | 0.402 | |
| Combined 9 sites | 10 | 10 | 10 | 10 | 11 | 9 | 10 | 10 | 10 | 10 | 10.5 | 11 | 11 | 11 | <0.001 |
Discussion
The chest X-ray is the commonest imaging modality performed and remains the most accessible in paediatric radiology for the evaluation of paediatric pneumonia.(3,8,16) The radiation dose from the chest X-ray is relatively low (0.02 mSv),(17) however the cumulative dose from multiple chest X-rays may be considerable.(3) Radiographic errors in paediatric chest X-rays are highlighted because they contribute to increasing the difficulty in making a diagnosis, and are more likely to be unsatisfactory in paediatric patients due to incorrect exposure factors, poor positioning and poor immobilization.(2,18,19) Such errors can result in an increased radiation dose due to the need for repeat imaging.(2,8)
In our results of chest X-ray quality assessment in children for diagnosis of pneumonia collimation performed the worst of the 6 parameters, with 5 out of the 9 sites being graded sub-optimally for this. In this group of 5 sites 51%-75% were graded as good, 24%-39% as fair, 1%-11% as bad for collimation.
These findings are consistent with the findings by Hlabangana et al. who conducted a chest X-ray quality assessment study in 438 children over a 4 month period at a hospital in South Africa with no paediatric trained radiographers.(3) This study also found that the most common error was poor collimation consistent with the results of the current study.(3) This error was also found in a study by Alt et al. who found that paediatric chest X-ray collimation, patient centring and patient positioning was insufficient in both departments with or without paediatric radiographers and radiologist in children younger than 5 years.(1)
The two sites with the best results Dhaka (Bangladesh) and Kilifi (Kenya) scored above 80% for all 6 parameters. While both sites have digital X-ray units, these sites do not have paediatric trained radiographers, children are X-rayed in the same department as adults and Kilifi (Kenya) does not have an onsite radiologist. In Kilifi (Kenya) radiographers have to routinely sign their name against all plain radiographs they perform. This may increase accountability when individual quality assessment feedback is given. In Dhaka (Bangladesh) site all PERCH chest X-rays were read for diagnostic and QA purposes by the PERCH study clinicians and feedback on quality was given at regular intervals to the radiographers. These factors may have contributed to these 2 sites performing optimally.
Three of the 9 sites Matlab (Bangladesh), Johannesburg (South Africa) and Nakhon (Thailand) showed a statistically significant improvement in chest X-ray quality over the 14 month period.
Johannesburg (South Africa) scored sub-optimally for exposure. This is consistent with the study by Gallet et al. who assessed all plain radiographs performed in the department over a 5 year period for 13 quality assessment parameters.(18) The authors found that overexposure to be the commonest error in all radiographs. Feedback to the radiographers from the PERCH study chest X-ray quality assessments, and rotating general radiographers to the paediatric radiology department to be trained by radiographers experienced in imaging of children during the course of this study could have accounted for the statistically significant improvement in the Johannesburg (South Africa) site.
Nakhon (Thailand) scored sub optimally for collimation as clinician's routinely request babygrams or chest X-rays to include the abdomen for children presenting with clinical pneumonia. During the course of this study clinicians were educated on ALARA principles and the increased risk for radiation-induced cancer in children compared to adults.(1,2,4) A modification in X-ray request forms from clinicians to only include the chest and avoid babygrams could have led to the statistically significant improvement in chest X-ray quality at this site. Another reason for the chest X-ray quality improvement is that this site converted from an analogue to a digital X-ray unit 6 months into the study.
In this study, none of the 9 sites showed a significant worsening in chest X-ray quality over the 14 month period. Hlabangana et al. showed statistically significant improvement in the quality of chest X-rays in children under 5 years, immediately after a poster intervention. However, this improvement was not sustained as they showed a significant decline in quality of chest X-rays 2 months after the intervention.(3) Thus the improvement in X-ray quality can only be sustained with regular, consistent QA and quality improvement initiatives as demonstrated in the current study.
This study was performed in sick children, hospitalized for WHO defined severe or very severe pneumonia, hence technical difficulties in obtaining chest X-rays in acutely ill children which have not been previously described in the literature may have played a role in this study. Furthermore unlike adult practice where a poor quality radiograph may be repeated, in paediatric practice a poor quality radiograph is often accepted, to avoid the increased radiation dose to the patient from repeat exposures. In busy paediatric wards in resource limited settings it is often difficult to arrange for a repeat visit to the radiology department.
Matlab (Bangladesh) and Bamako (Mali) had a significant number of chest X-rays scoring fair in processing. During the course of the study it was noted that digital X-ray unit in Bamako (Mali) needed to be cleaned and serviced. A number of chest X-rays had linear lines suggestive of pressure marks from the processor. The delays in timely repair of the faulty equipment limited the quality of chest X-rays in Bamako (Mali). In Matlab (Bangladesh) the X-ray scanner machine did not have a transparency unit, which resulted in poor quality of chest X-rays that were scanned from analogue to digital format. A large flatbed scanner (Epson 10000XL) was borrowed from the Thailand site approximately 1 year into the study to improve chest X-ray processing quality.
Limitations
This study did not evaluate the impact of the quality of chest X-rays in making a radiological diagnosis of primary end point pneumonia, other infiltrate or normal chest X-ray.(20)
One paediatric radiologist reported chest X-ray quality through the customized report formatting; hence this study is unable to determine inter observer variability. However, the strength of the study is that the same external paediatric radiologist reported chest X-ray quality prospectively from each of the 9 sites over the course of the 14 month study period.
We were unable to analyse if specific clinical features were predictive of poorer chest X-ray quality, due to limitations in the study design.
From the monthly uploads to the EMMES Corporation three of the 9 sites used analogue X-ray units and these sites scanned printed chest X-rays to a digital format, which could account for the disparity in chest X-ray quality.
A variable number of chest X-rays had quality assessment over the 14 month period in each of the 9 sites. The site specific limitations and challenges are reported in Supplementary Table 5.
Site Specific Limitations and challenges in optimizing image quality
| Site (Country) | Radiology Department Site Limitations |
|---|---|
| Bamako (Mali) | Faulty equipment required servicing and delays in timely repair limited quality of CXRs. For the first 6 months all PERCH CXRs were assessed weekly for diagnostic and quality assessment, this was changed to daily during the course of this study. |
| Basse (The Gambia) | Breakdown of the digital X-ray unit resulted in the use of back-up analogue X-ray unit with subsequent digitization of films. PERCH study site clinicians changed during study period, hence study clinicians had varying competencies in CXR quality assessment. Reading of all CXRs for diagnostic and quality assessment done by study clinicians only commenced 4 months into the study. |
| Dhaka ICDDR B (Bangladesh) | Plain film radiographs were not routinely read by radiologist. |
| Dhaka Monowara (Bangladesh) | Private hospital where a broader pool of radiographers rotates without dedicated radiographers for paediatric imaging. PERCH CXR quality assessments were not routinely directed to the radiographers at this site. |
| Johannesburg (South Africa) | Radiographers have a very high workload. Dedicated, trained radiographers in paediatric radiology department available only during working hours ie: Monday to Friday 8am to 4 pm. PERCH feedback was only directed to radiographers in paediatric radiology department. Large number of analogue portable CXRs performed on children due to significant distance of the radiology department from paediatric wards. Despite transitioning to a digital X-ray unit, for first year CXRs had to be printed and scanned as no software to store CXRs digitally. |
| Kilifi (Kenya) | Radiographers found positioning and imaging of very young children a challenge and did not have a patient immobilization device. This may have contributed to poorer positioning and collimation young children compared to other parameters. |
| Lusaka (Zambia) | Children are X-rayed in the same radiology department as adults and there are no radiographers dedicated to imaging of children. All CXRs that were performed in the paediatric campus were done with a portable analogue X-ray unit which may have impacted on CXR quality especially with exposure and collimation. Dirty or damaged screens also led to artefacts like scratches on CXRs. |
| Matlab (Bangladesh) | One radiographer who performed X-rays on adults and children An analogue X-ray facility, with some limitations to maintained quality. The X-ray scanner machine did not have a transparency unit, a large flat bed scanner Epson 10000XL was borrowed from the Thailand site approximately 1 year into the study to improve CXR processing quality. |
| Nakhon Phanom (Thailand) | Clinicians routinely requested babygrams or CXRs to include the abdomen as part of routine clinical practice |
| Sa Kaeo (Thailand) | Clinicians routinely requested babygrams or CXRs to include the abdomen as part of routine clinical practice |
Recommendations to Ensure Good Quality Chest X-rays with Dose Optimization in Developing Countries without Paediatric Radiographers and Paediatric Radiologists
- 1.
Quality assurance programs are paramount in radiology departments and do not need to be facilitated by radiologists but should be ongoing to ensure sustained compliance with optimised radiologic examination.
- 2.
Having a core group of radiographers trained and dedicated to radiographic imaging of children is very important especially in radiology departments where children are imaged with adults.
- 3.
Pairing radiographers with experience in imaging of children with less experienced radiographers is important to train junior staff in selecting optimal imaging parameters.
- 4.
Monthly random analysis of a set of plain films with feedback to radiographer's can be useful and may result in sustained trend of improvement
- 5.
Radiographers signing against each X-ray performed may improve accountability and allows for personalized feedback so radiographers
- 6.
Education of clinicians on the ALARA principles in children and Image Gently campaigns may enable optimization of request forms to prevent overexposure of children example babygrams.
- 7.
Where possible, all plain films should be reported by radiologists with real time feedback to radiographers
- 8.
Stream line workflow to avoid analogue portable X-rays which have greater technical difficulty especially for inexperienced radiographers
- 9.
Ensure all radiographic equipment is functioning optimally with daily routine checks. A medical physicist can choose the appropriate receptor, ensure adequate filtration and processing of images.(7)
- 10.
Collimation may be poor even in departments with paediatric trained radiographers due to the use of wide collimation in moving, uncooperative children to prevent repeat imaging when the area of interest is outside the field of view. Hence thyroid and gonadal shielding is very important when imaging children.(7)
Conclusion
Chest X-ray quality optimization is important for accurate diagnostic purposes. We found that collimation performed the worst of the 6 chest X-ray quality assessment parameters, in keeping with previous findings in the literature. This limitation maybe difficult to overcome as wide collimation is used with moving and uncooperative children to avoid repeating X-rays. Education of clinicians in ordering the most suitable radiological test and avoiding baby-grams is important.
In this study chest X-ray QA intervention applied in each of the 9 sites showed a significant improvement in chest X-ray quality in some sites and none of the other sites showed a worsening in chest X-ray quality.
Recommendations from this study include pairing radiographers experienced in imaging of children with less experienced radiographers, to train junior staff in optimizing chest X-ray quality. Where possible, all radiographs in children should be reported by radiologists with real time feedback on quality to radiographers. Ensuring that all radiographic equipment is functioning optimally is important to obtain good quality radiographs. The findings from this study are important for novel research on the use of artificial intelligence in improving paediatric chest X-ray quality.